第三章:院內型肺炎
3-4 治療評估及診斷流程
重點提要
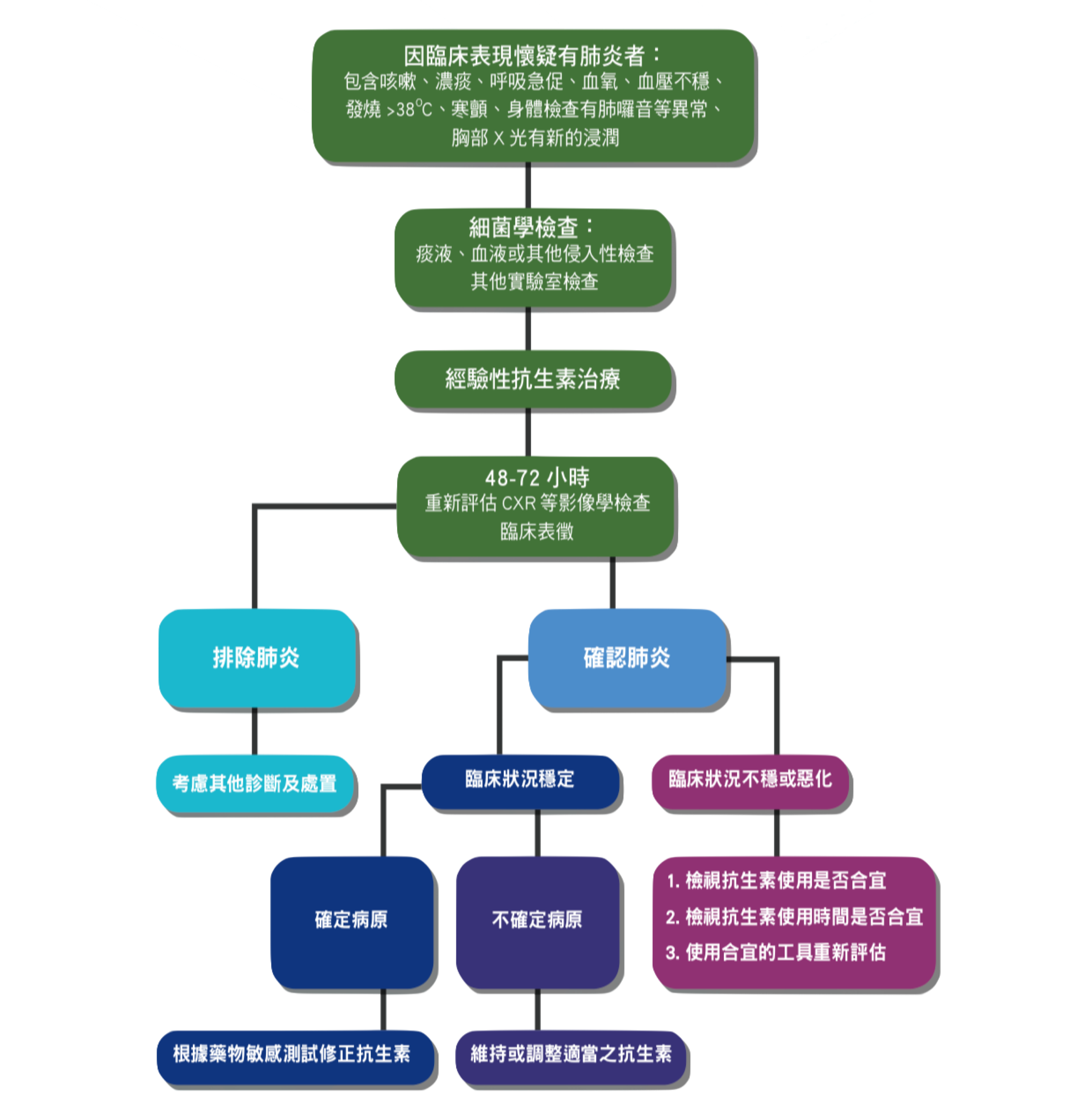
本節說明院內型肺炎診療流程,以及治療穩定與失敗的定義。治療失敗為經抗生素治療 48~96 小時後,臨床情況惡化或生命徵象不穩定,應重新評估,內容包括抗生素使用是否合宜,應考量有無抗藥性、藥物動力學(pharmacokinetics, PK; pharmacodynamics, PD)、合併症、抗生素使用時間及共病等問題,並運用影像、微生物檢驗及支氣管鏡檢查協助判斷。
主編:詹明澄
副編:施智源
一、初始治療穩定(clinical stability)的診斷標準
加入書籤
符合下列條件六:體溫:< 37.8°C;心跳 < 100/分鐘;呼吸速率 < 24/分鐘;收縮壓 > 90 mmHg;血氧飽和度 > 90%(FiO2:21%);能經口進食;意識正常 [1]。
二、院內型肺炎及呼吸器相關肺炎(HAP/VAP)治療失敗定義
加入書籤
符合院內型肺炎定義之住院患者,經抗生素治療 48~96 小時後,因臨床情況惡化(clinical deterioration)或生命徵象不穩定(如持續性發燒、休克、呼吸情況惡化甚至衰竭或死亡);或一開始臨床情況進步,之後臨床情況惡化 [2]。
三、處置建議
加入書籤
針對院內型肺炎(Hospital Acquired Pneumonia, HAP)及呼吸器相關肺炎(Ventilator-Associated Pneumonia, VAP),產生治療失敗(treatment failure)時,我們可以從下列幾個方向來思考 [3][4][5][6][7][8]。
(一)檢視抗生素使用是否合宜(Appropriate antibiotics)
- 當培養有菌種時且包含多重抗藥性(multiple drug resistant, MDR),應重新檢視 MDR 的相關議題。產生 MDR 的風險因子跟下列因素有關係 [7][8]。
- 發生肺炎時間點(早期或晚期)
- 先前是否使用過抗生素
- 是否合併相關共病及罹病
- 是否有出現器官衰竭情形(organ failure)
當上述的條件都成立時,代表出現 MDR 的風險最高。
- 當培養仍陰性時,可重新送驗並檢視有無其他感染,或病人是否有合併其他共病(comorbidity)如心臟衰竭、肺栓塞,或其他器官共病 [3]。
- 建議需考慮藥效動力學(pharmacodynamics, PD)及藥物動力學(pharmacokinetic, PK)之影響,有可能是藥物濃度不足造成治療失敗。一般使用 aminoglycosides 或是萬古黴素(vancomycin)時可考慮監測藥物濃度 [7]。
- 考慮是否有次發性感染或合併其他感染(secondary infection or co-infection),除細菌外,也應考慮黴菌、結核菌或其他少見菌種(包含病毒)的合併感染 [4]。
(二)抗生素使用時間是否合宜(Appropriate duration of antibiotics use)
- 一般而言,治療 HAP 或 VAP 使用抗生素的時間約為一週 [5][7]。
- 當有下列情形需調整抗生素使用時間 [7]:
- 病人因素:免疫不全病人例如白血球低下(neutropenia)或幹細胞移植(stem cell transplant)、膿胸(empyema thoracis)、肺膿瘍(lung abscess)、肺有開洞及壞死性肺炎(necrotizing pneumonia)等。這時會延長抗生素使用時間。
- 病原菌因素:多重抗藥菌種,如綠膿桿菌(Pseudomonas aeruginosa)、碳青黴烯類抗藥不動桿菌屬(Carbapenem-resistant Acinetobacter spp.)和碳青黴烯類抗藥腸內菌屬(Carbapenem-resistant Enterobacteriaceae)。
- 抗生素因素(Antibiotics issue):臨床上治療 HAP 或 VAP 時,第一線用藥遇到抗藥的菌種時,為了避免進展到治療失敗,進而需使用黏杆菌素(colistin)或老虎黴素(tigecycline)作為第二線用藥時,此時抗生素的使用時間應根據臨床狀況作調整及適度延長,而非拘泥於一週的治療時間。
(三)使用合宜的工具重新評估(Appropriate tests and tools for re-evaluation)
- 可考慮的介入措施,包含影像、微生物檢驗及支氣管鏡檢查。
- 影像檢查方面:一般首選是以胸部 X 光片為主,當臨床上有需要時可考慮胸部電腦斷層影像檢查。當有懷疑氣管內病灶時(endobronchial lesion),可考慮施行支氣管鏡檢查。
- 微生物檢驗方面:建議再重新採檢及取樣,當臨床檢體不易取得時可搭配支氣管鏡檢驗來協助收集檢體及取樣。
- 關於 C-反應蛋白(C-reactive protein,CRP)及前降鈣素(procalcitonin,PCT)檢驗:
圖 3.4.1 院內型肺炎及呼吸器相關肺炎(HAP/VAP)診斷流程及處置
四、參考文獻
加入書籤
M Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults andell LA, Wunderink RG, Anzueto A, et al.. Clin Infect Dis 2007;44(Suppl 2):S27-72. ↩︎
Ramirez J, Dartois N, Gandjini H, et al. Randomized phase 2 trial to evaluate the clinical efficacy of two high-dosage tigecycline regimens versus imipenem-cilastatin for treatment of hospital-acquired pneumonia. Antimicrob Agents Chemother 2013;57(4):1756-62. ↩︎
American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005;171(4):388-416. ↩︎ ↩︎
Cawcutt K, Kalil AC. Pneumonia with bacterial and viral coinfection. Curr Opin Crit Care 2017;23(5):385-90. ↩︎ ↩︎
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016;63(5):e61-e111. ↩︎ ↩︎ ↩︎
Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med 2017;43(3):304-77. ↩︎
Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur Respir J 2017;50(3). ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wilke M, Grube R. Update on management options in the treatment of nosocomial and ventilator assisted pneumonia: review of actual guidelines and economic aspects of therapy. Infect Drug Resist 2013;7:1-7. ↩︎ ↩︎